October 15, 2015
The slow-moving tsunami that is antibiotic resistance invokes the specter of ordinary people a few generations from now being struck down by once-curable common infections: septicemia that starts with a paper cut, bronchitis that turns into fatal pneumonia. These events were common before the advent of antibiotics and have now become the boilerplate impending dangers of antibiotic resistance. Estimates have been made of just how many lives could be lost. To those scenes are added the common refrain that growing antibiotic resistance threatens safe surgery and chemotherapy for some cancers.
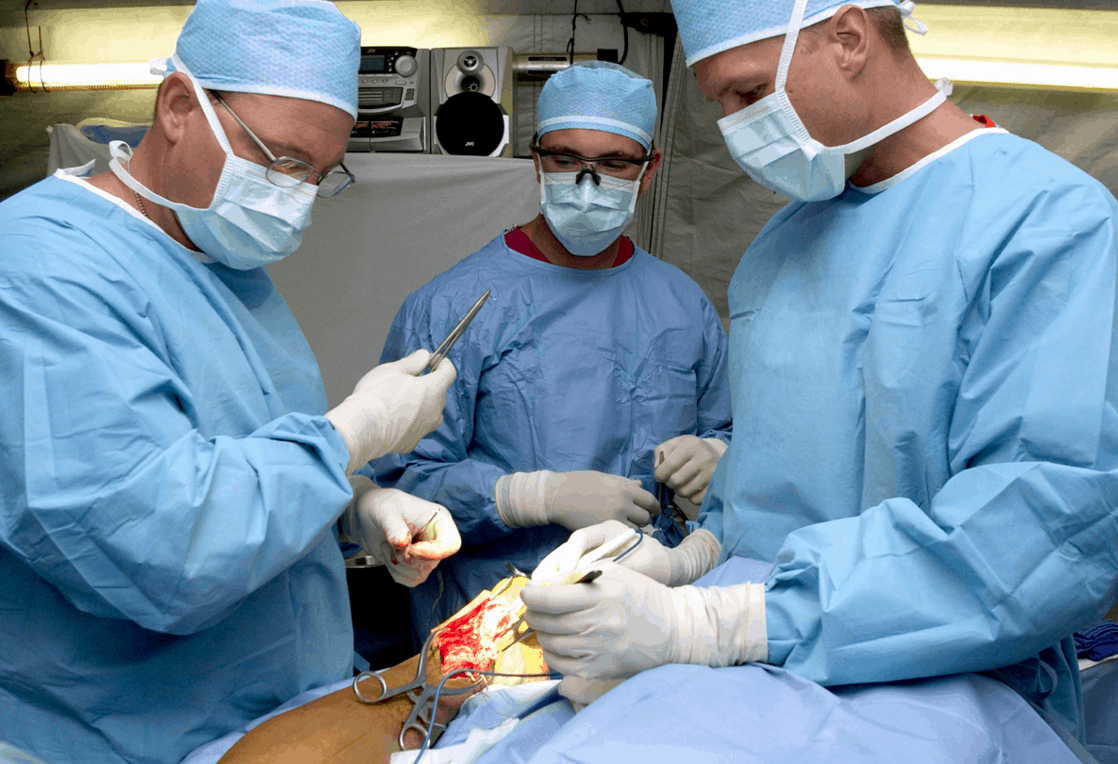
This, too, has become boilerplate: the direct connection between antibiotic resistance, surgery and cancer. Prophylactic antibiotics before surgery prevent surgical-site infections, which were much more common before this practice began. Organ transplants are a particularly difficult case: they require long-term immunosuppressive drugs to prevent rejection of transplanted organs, which leaves patients open to bacterial invaders. Organ transplants are impossible without antibiotics. And many cancer treatments—especially for leukemias and lymphomas that involve blood and lymph cells—suppress the immune system, leaving patients vulnerable to infection. Antibiotics protect them.
These risks have been talked about for years, but no one had quantified them before now: how many people faced with surgery or cancer treatment might be affected by growing antibiotic resistance? At what cost? A group of CDDEP researchers has made the first serious estimate, which appears in the journal Lancet Infectious Diseases this week.
Their estimates do not cover all surgeries and immunosuppressive chemotherapy, but they do cover the 10 most frequent surgeries in the United States—from cesarean section at number one to hip fracture surgery at number 10—and chemotherapy for blood-borne cancers (leukemias, lymphomas, myeloma). Using all of the reliable published literature, they began by estimating “both the effects of antibiotic prophylaxis on infection rates and the effects of antibiotic resistance on infection rates for different procedures.”
The rates of infection after surgery with no antibiotic prophylaxis vary enormously from procedure to procedure, but are not trivial in any of the cases. Not surprisingly, the highest rate is for colorectal surgery—the colon is filled with bacteria, which can easily escape into surgical wounds. Without antibiotics, a full 39 percent of patients develop post-operative infections, and of these, 43 percent are resistant to the antibiotic recommended for prophylaxis.
It is clear that antibiotic resistance is already having an impact on these procedures. What happens when the resistance rates increase, as they are doing in the United States? My colleagues calculated the expected effect. Here is what they found for a 30 percent reduction in the efficacy of antibiotic prophylaxis, a not unreasonable expectation: 120,000 additional infections per year in the United States among surgical patients and patients getting chemotherapy for blood-forming cancers.
Healthcare-associated infections are not just inconvenient and expensive: some are deadly. The same 30 percent reduction in efficacy could result directly in well over 6,000 additional deaths each year, most of them colorectal surgery patients. That is a conservative estimate, and includes only seven of the 10 surgical procedures, because no reliable information was available to make estimates for the remaining three.
That doesn’t count the thousands of patients likely to forego live-saving organ transplants or other surgeries because they may no longer be kept safe from infections. And the overall increase in infections would increase costs dramatically, in the form of newer, more expensive antibiotics and longer hospital stays.
What might help? Antibiotic stewardship and infection control in hospitals can help reduce surgical and cancer-related infections, making reliance on antibiotic prophylaxis somewhat less important. But even the best practices leave patients vulnerable. We could use more advanced (and much more expensive) last-resort antibiotics routinely for prophylaxis, but that will just drive up resistance to those antibiotics..
The best investment could be an increase in our attention to and spending on antibiotic stewardship and conservation, which would likely have a huge payoff in lives and dollars saved by slowing the rate of increase of antibiotic resistance.
My colleagues have now put numbers to the boilerplate of surgery and cancer treatment. Will we simply watch while their predictions unfold, or will we step up our efforts to preserve antibiotic effectiveness?
Hellen Gelband is CDDEP’s Associate Director for Policy.