May 30, 2012
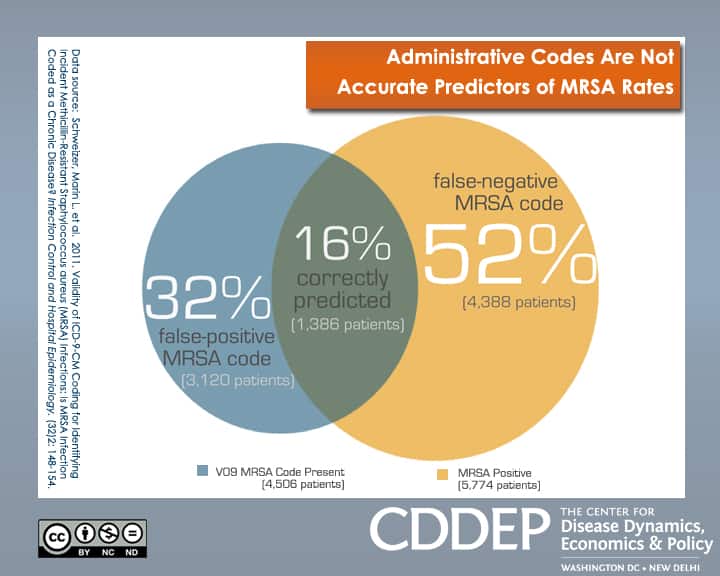
Researchers and healthcare agencies often rely on administrative information to track rates of infections with the antibiotic-resistant bacteria called MRSA (methicillin-resistant Staphylococcus aureus). Despite of frequent revisions to coding guidelines, billing data is subject to human error and cannot capture the full complexity of clinical care. The graphic shows that between 2001 and 2007 almost one-third of patients discharged from three large hospitals received an administrative code for a drug-resistant infection (called the V09 code) even if lab results showed they were not infected with MRSA during their hospital admission. Conversely, over half of the patients received a “false-negative” MRSA code meaning they were not assigned the V09 code even though they test positive for MRSA. The inaccuracy often occurred because the patient had a prior history with the condition, and the coder would treat MRSA as if it were a recurrent problem such as diabetes and other chronic diseases.
Although improvements were introduced in 2009 to define MRSA more narrowly, the updated codes have yet to be verified. In addition, since a large share of errors were linked to misinterpretation of the medical record by the coder, it is likely that the overuse of MRSA codes persists. Despite the convenience of ICD-9 codes for disease surveillance, their primary use is for billing and researchers should ideally test the validity of such data against actual patient charts.