
October 08, 2015
The Presidential Advisory Council on Combating Antibiotic-Resistant Bacteria held its inaugural meeting in Washington, D.C on September 29, 2015. The meeting, which was webcast to the public, included presentations by infectious disease experts from across the United States. The conference was positive and upbeat and showcased the many initiatives the United States has under way to confront the epidemic of antimicrobial resistance.
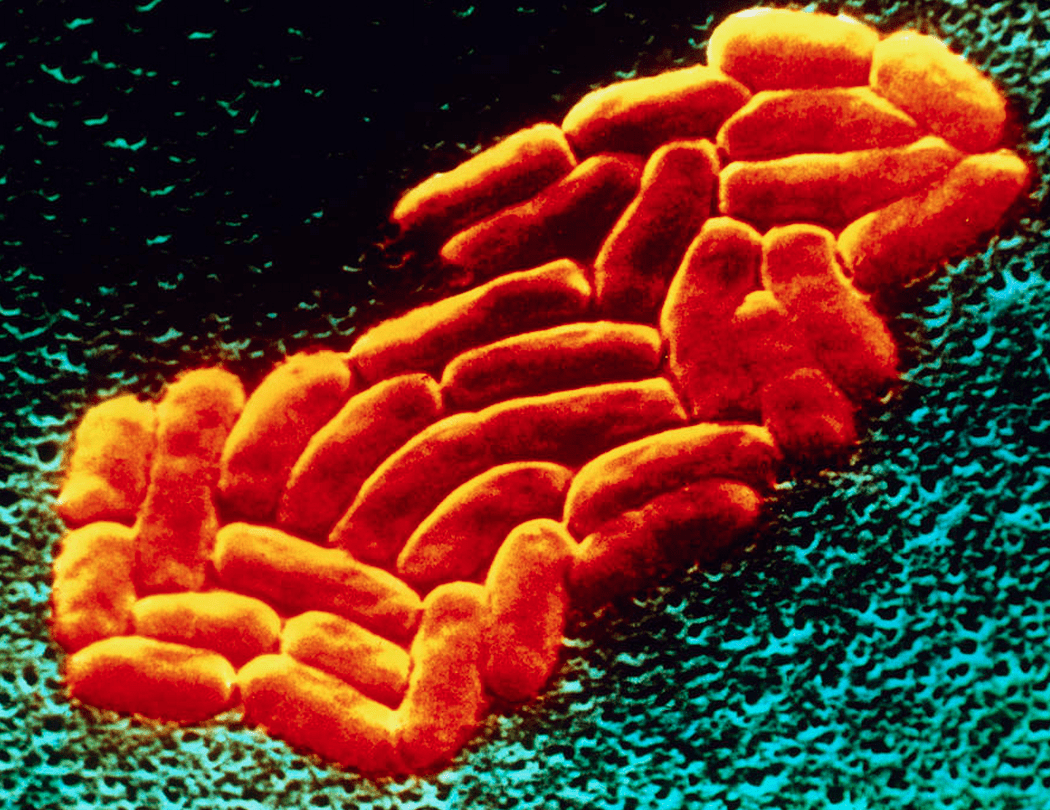
One of the most impressive presentations was from a little-known agency called BARDA, the Department of Health and Human Services’ Biomedical Advanced Research and Development Authority. Its mission is to develop and stockpile agents for use in public health emergencies.[1] BARDA has had 21 products approved by the FDA, and is currently supporting the development of six antibiotic products designed to quell highly resistant bacteria that are spreading around the globe, which military members are exposed to ever more frequently in overseas deployments. Among the most dangerous are carbapenem-resistant Enterobacteriaceae (CRE), which thrive even in the face of carbapenems, considered “last-resort” antibiotics.
I’m not laying blame on any one or any agency; the allotted resources are scant and the expansion of any of these tracking systems would require a massive increase in operating budgets. At this point, the U.S. Congress has been unwilling to fund a truly workable tracking system. And of course, even if the system is built, it may not be used. Voluntary reporting has a dismal track record in the United States. Mandatory reporting will also be needed.
In the case of CRE, the lack of a comprehensive and uniform reporting system has created a situation that has placed the United States in the embarrassing predicament of detecting the CRE epidemic spread by endoscopes nearly two years after it was detected in Europe.[4]
The 21st Century Cures Act was passed by the U.S. House of Representatives in July 2015. This bill, like much of the ongoing discussion in medicine on how we should confront this epidemic, stresses the need for new antibiotics. We’ve already seen that BARDA has a number of antibiotics under development or the in commercial pipelines that should be effective against some of the most resistant strains. The real question, however, is: Will any new antibiotic be used sparingly—only when truly needed—and its effectiveness conserved, or will we let history repeat itself with excessive use and the rapid development of bacteria resistant to it?
The 21st Century Cures Act does little to promote the stewardship that is the ultimate weapon against antibiotic resistance. What is missing is a clear statement that the development of last-resort antibiotics is just that: drugs that are exclusively to be used as a last resort, when there are no alternatives. The provisions in the bill could easily be construed as allowing the promotion of antibiotics based upon their cost effectiveness—i.e. if a drug is cost-effective, it should be used.[5] Instead, federal support should dictate that these antibiotics be reserved and used only when absolutely necessary.
Tracking and publicly reporting provider prescribing patterns should also be an element in safeguarding antibiotics of last resort. Provider utilization data are regularly collected by the drug industry for the purpose of marketing. Why can’t we also have it to safeguard the public’s health?
Accessed on Oct. 3, 2015 from: http://www.usatoday.com/story/news/2015/08/05/duodenoscope-infections-not-reported/29988165/










{kind=link}