January 23, 2013
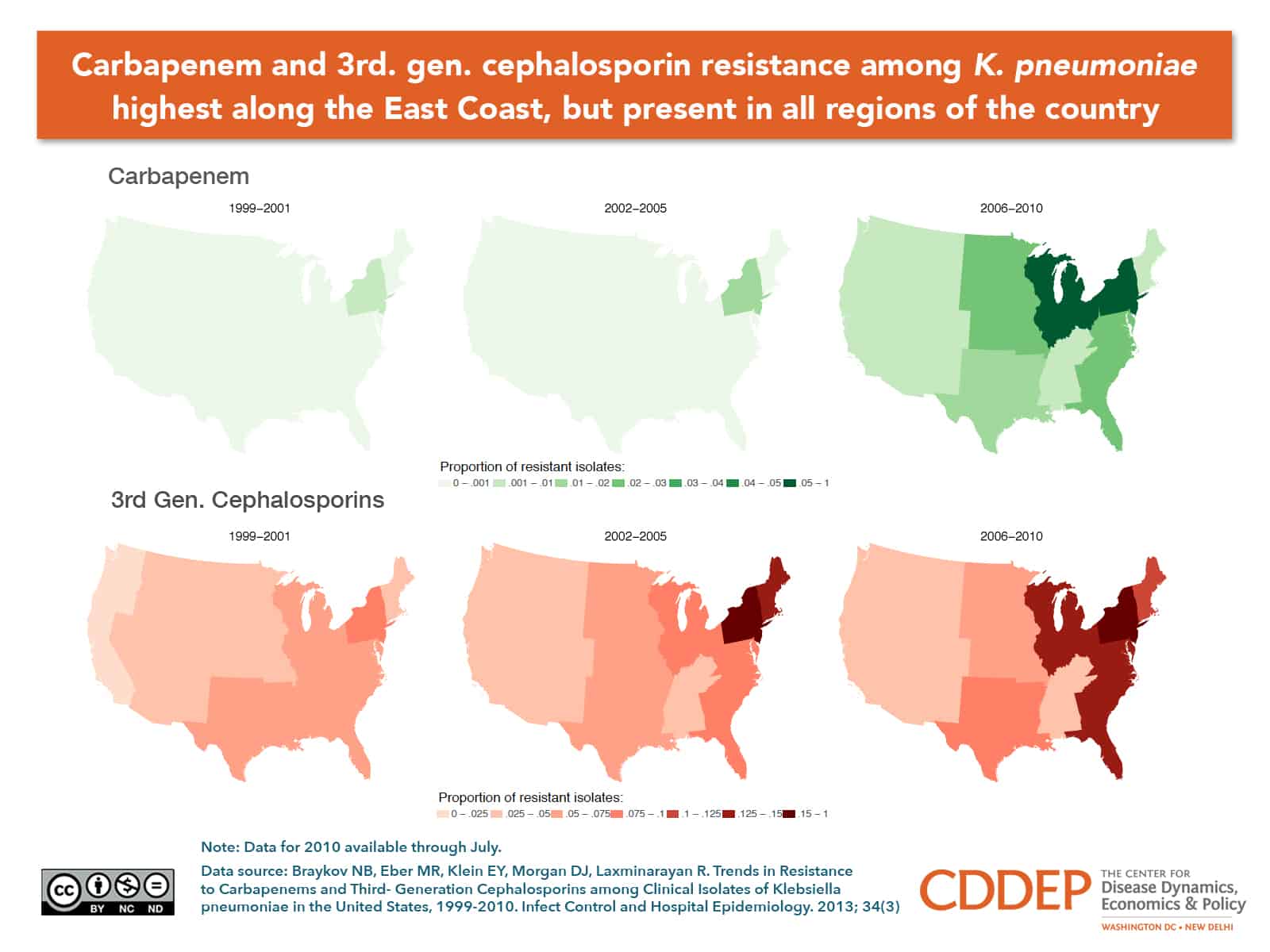
The maps show the geographic spread of K. penumoniae isolates exhibiting resistance to third-generation cephalosporins (G3CRKP) and carbapenems (CRKP) between 1999 and 2010. Resistant phenotypes were more endemic in the Eastern part of the country, particularly the Middle and South Atlantic Census divisions. CRKP emerged in the New York metropolitan area in the mid-2000s and spread into other geographies, particularly East North Central states. For both phenotypes, it was lowest in the West and highest in the Northeast, followed by the South Atlantic region. The percentage of G3CRKP isolates was highest in the Northeast and initially grew faster than in other regions, peaking in 2005. For both phenotypes, resistance trends in the West remained almost flat by comparison with other regions, but still increased. Recent reports confirm CRKP is endemic in Los Angeles County.
The observed national rise in CRKP is particularly disconcerting for several reasons. First, CRKP infection is associated with a fatal outcome in 47% 57% of cases. Second, treatment is limited to older antibiotics known for high kidney toxicity a limitation that highlights the urgent need to develop drugs active against Gram-negative bacteria. Third, the ability of resistance-encoding genes to spread through plasmid transfer enables the spread of resistance to related species like E. coli, a transfer that may occur even in the same patient. Finally, CRKP genes may escape detection in routine laboratory testing. The epidemiology of carbapenem-resistant bacteria thus has the potential to replicate the endemic spread of MRSA beyond hospitals and into the community.